Multi-Unit Abutments are the engineering solution that transformed full-arch implant prosthetics into a standardized, reproducible protocol. In an All-on-4 or All-on-6 rehabilitation, the underlying implants are placed at varying angles dictated by available bone — the two anterior implants may be straight, while the posterior implants are deliberately tilted at 30–45° to avoid the maxillary sinus or mandibular nerve and maximize prosthesis support length. Without MUAs, connecting a single rigid prosthesis to four implants at radically different angles would create severe stress concentration at the connections. The MUA solves this by creating a gingival-level platform above each implant where the prosthesis connects — allowing the MUA angle to compensate for the implant angle and producing parallel connection points at a uniform height, regardless of what the implants are doing below the gumline.
The Neodent GM Multi-Unit Abutment engages the Grand Morse® 16° internal cone at the implant level. This deep conical seating generates compression between the implant and abutment — the same mechanism that gives the GM system its anti-rotation stability and biological seal. At 32 N.cm, the MUA is locked to the implant with negligible micromovement and a tight seal at the interface. Above the shoulder, the MUA presents a standard prosthetic tube compatible with Neodent GM bar components, screw-retained cylinders, CAD/CAM milled frameworks, and prefabricated prosthetic components — the complete ecosystem of full-arch solutions. The MUA is seated once at surgery and is typically left permanently in place as the stable long-term anchor for the overlying prosthesis.
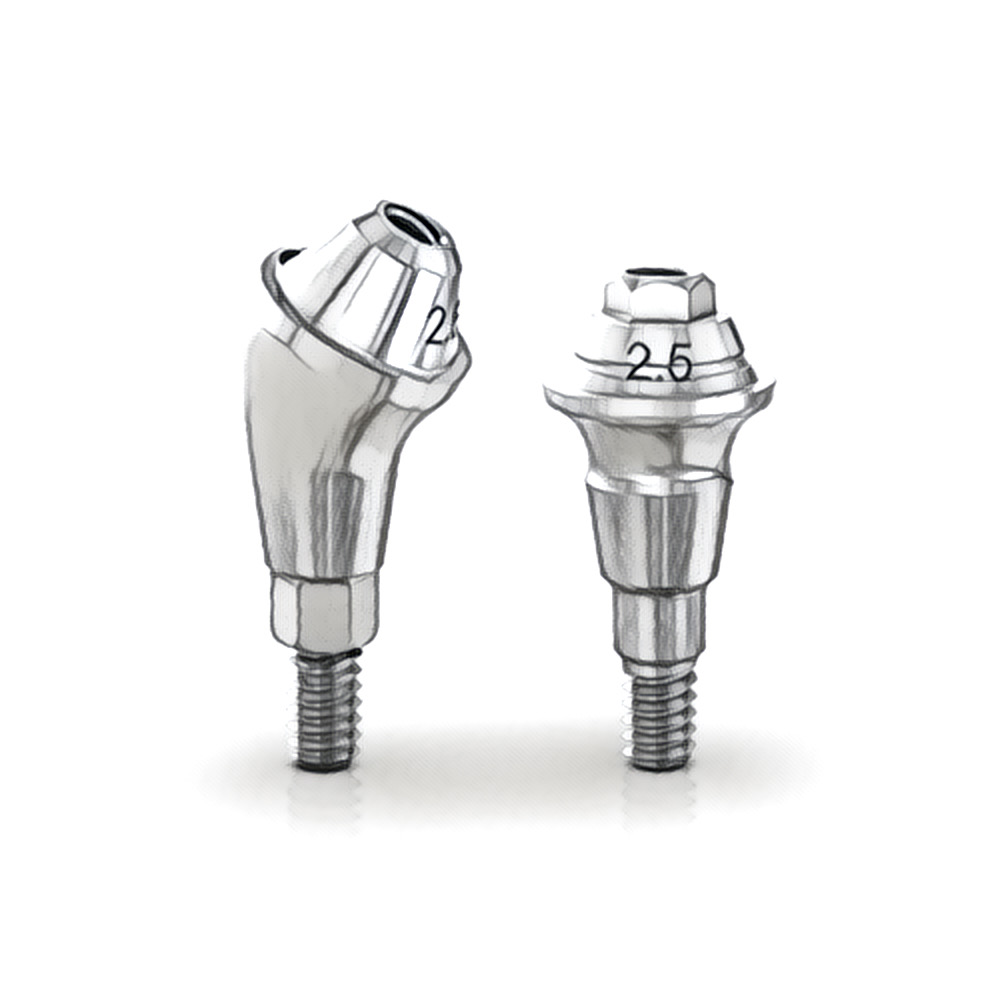
The three available angulations (0°, 17°, and 30°) address the three primary clinical scenarios in full-arch rehabilitation. The 0° straight MUA is used on axially placed anterior implants where no correction is required. The 17° angled MUA is the workhorse of All-on-4 — used on moderately tilted posterior implants. The 30° angled MUA addresses the most angulated positions: maximally tilted posterior implants, pterygoid implants, and zygomatic implants, where the body angle relative to the prosthetic plane exceeds 25°. Together, these three angulations allow the surgeon and prosthodontist to achieve prosthetic parallelism in virtually any full-arch implant configuration without custom or patient-specific components.
The four gingival heights (1, 2, 3, and 4 mm) serve an equally critical function: they allow the MUA shoulder to be positioned at the ideal level relative to soft tissue. Implants at different sites will have varying distances from their platform to the gingival surface. Selecting the correct gingival height ensures the prosthetic connection emerges cleanly at or just above the gingival margin at every position — creating a hygienic, accessible interface that patients can maintain long-term. An incorrectly selected gingival height (too deep) creates a subgingival connection zone that accumulates plaque and drives peri-implant mucositis.